Confronting Commercialization of Healthcare
Recently I came across an interesting book, “The People’s Health Sourcebook”. Section 5 of this book was of particular interest to me, I have used its title as the title of this article, I am a healthcare architect with by and large corporate clients.
I am encouraged to quote extensively from the book by the authors themselves, they say:
“Any part of this book or the entire book may be copied or translated or used in any way provided it is not used for profit or commercial purposes.”
Well I will get paid a few hundred rupees for this article; I hope the authors will not grudge me that. I would just like to examine their thesis in the light of my experience of working closely with corporate healthcare providers in designing their hospitals. Being an architect and a very visual person myself I am delighted to re-present the very good visuals they use to make their point, the first one of which immediately follows:
The text following this is:
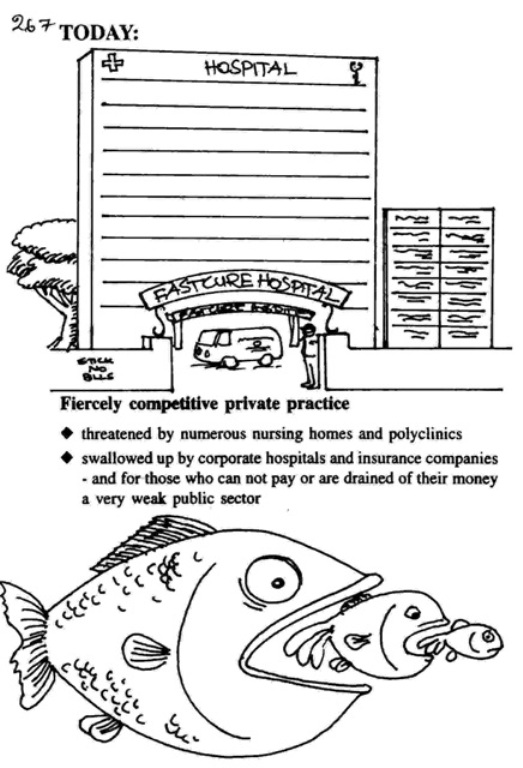
Only 22% of the health expenditure is public funded in India as compared to 44% in the US, or 95% in countries like Sweden or 75% in all the market economies of the world taken together.”
And then Uncle Sam tells us:
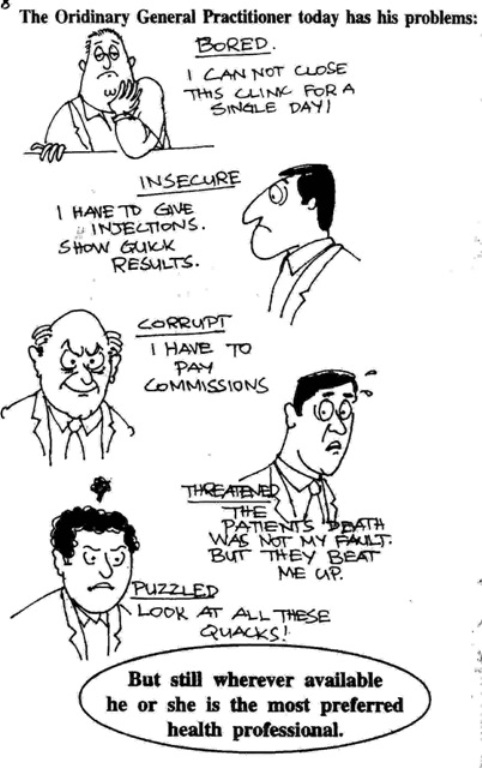
“But there are lots and lots of problems with this simple solution: What are the popular causes for dissatisfaction against doctors and the delivery of health care in India today?
We have now half a dozen very cynical doctors, grimacing…
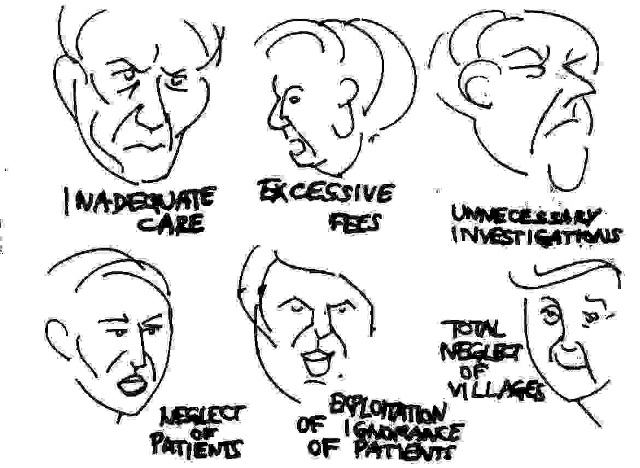
“These causes are leading to an increasing alienation of the community from the Medical profession, which is a very unhealthy trend.”
“Yesterday, all my troubles seemed so far away…” warbled the Beatles. Little did they know they were singing about Indian healthcare delivery systems.
My family doctor as a child was very much a friend of the family. Much more than a friend really, he was treated as a demi-god…The medicine was dispensed in little paper twists, and seemed to be a mixture of some or all of half a dozen powders for any illness…
The corporate hospital below is architecturally unappealing, but the point gets made: a drain for money…(don’t miss the security guard). Quickfix hospital indeed.
Ah, the problems of the GP…but he bears them manfully, he is most preferred after all.
The breakeven analysis, a French phrase for something unmentionable…guess I’m incurably foulmouthed. Let us pray to the gods that be that nothing ever breaks even, perish the thought!
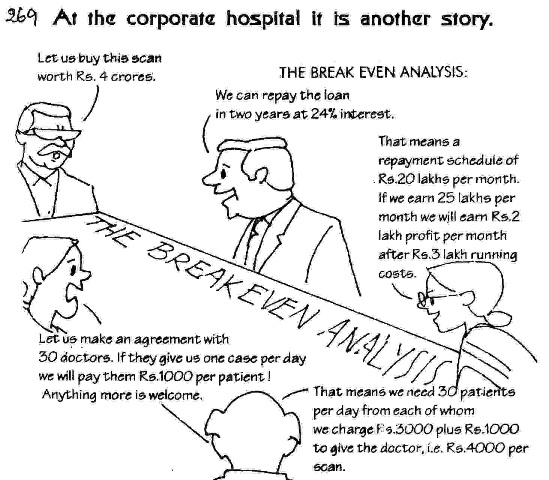
The book goes on to say:
“A corporate hospital is run like an industry! It is run to maximize returns on investment. The number of people who need investigation will invariably be less than that needed to break even – especially as more and more hospitals will open. Where there is a high return of investment in any sector in a market economy, more units of that type develop. However this will not push down costs or promote efficiency. It will rather promote more unnecessary investigations, unnecessary hospitalization, unnecessary surgeries and unnecessary referrals. Some of these are done as malpractice. But a greater trend is to shape modern medical science so that there is more and more “need” for investigations, hospitalization and surgery. For any other commodity if there is competition the price will stabilize around its value. But since no value is too high for human life, the ability to price is limitless. It is limited only by the ability of the consumer to pay.”
Strong words. I would, by and large, disagree. Let me tackle it point by point, and present my viewpoint on the rhetoric above.
An exclamation mark after industry indeed! “Maximize returns on investment”, do I need to wash my mouth out with soap again? What was wrong with the Indian mantra after Independence? Among other things, it set up a huge, inefficient public sector (including public healthcare) to which it denied autonomy of working; there were low to no “returns on investment” (excuse all this obscenity) and we had a poor capital-output ratio. It also pampered organized labor to the point where productivity became extremely low. All the rulers of our country did was institutionalize democracy, in the name of the poor. Indian socialism ended up doing very little for the poor. Ideology is not the solution, better management and more especially incentives to manage better, are.
A high return on investment in healthcare? To succeed in the 21st century, healthcare providers need to respond to the looming threat of competition and capitation. “…will not push down costs?” The impending advent of insurance and health maintenance organizations will usher in managed care. Where policy-led reform failed, market-led reform may succeed. The driving force in healthcare is going to be an economic message of managing care, managing cost, and managing clinical efficiency to create a sustainable healthcare delivery system for India. For us who are marketing design services, we can already see a shift in the customer. The customer in the past has been the hospital. More recently it is becoming the medical group and tomorrow’s customer will be the health network or even a HMO.
“Some of these are done as malpractice. But a greater trend is to shape modern medical science so that there is more and more “need” for investigations, hospitalization and surgery.” Sir, madam, the second is more than mere “malpractice”, it is paranoia on your part and megalomania on the part of the modern medical scientists engaged in this endeavor, if any are so involved. Both are pathological conditions and call for therapy.
“But since no value is too high for human life, the ability to price is limitless. It is limited only by the ability of the consumer to pay.” “Rhetoric” is defined by my Webster’s College Dictionary as ‘language skillfully used’. It goes on to also define it as the ‘undue use of exaggerated language; bombast.’ I submit that along with the evils of globalization we have also been given to learn the skills of shopping. A fool and his/her money will always part ways soon. We do not debate the actions of fools. Corporate hospitals target the well-to-do as customers; they got that way by being savvy about money matters. They pay for quality.
The economic risk of providing comprehensive services to a potentially large and eventually enrolled population will have to be managed by clinical integration and disease management. This is the reengineering of patient care. The design opportunity in this is not simply to make reengineered care clinically efficient, but to focus on the patient care experience and on the processes of achieving greater efficiency through improved engineering and facility design. The mantra is patient-focused care, not about providing spectacles by charging separately for the frame and each of the lenses.
As the kids nowadays say, “get real…”
947 thoughts on “Confronting Commercialization of Healthcare”