Grid-Shrinking as a means of Cutting Costs in Healthcare Facility Design: A Conversation
Hussain Varawalla Healthcare Architect
Syed Basharath Ali-CEO-Tameer Consulting Associates
Sameer Mehta Director-Projects-Hosmac India
Following are the proceedings of an email debate on whether shrinking the column grid in a proposed healthcare facility project would be an effective way of cutting costs.
Basharath Ali’s views on the matter were as follow:
- Shrinking of the grid results only in a corresponding decrease in slab area. The number of columns remains the same, and the minimal decrease in span does not lead to a corresponding decrease in column/beam cost as the area.
- The number of doors, windows, electrical points, gas points etc all remain the same.
- While the amount of flooring proportionately decreases, the walls and painting area do not.
- Facade costs remain almost the same as the height has not proportionately reduced.
In short, all individual items and everything in the vertical dimension are unchanged. Since the vertical dimension comprises 4 times more than the horizontal, this is not the most value-effective way of decreasing cost.
He opined that the cost of the project would decrease by less than 50% of the proportionate decrease in area. I think he was being polite, politically correct, trying not to upset the client!
The decrease in the more intangible values for the healthcare facility in grid cutting is tremendous and is difficult to quantify without getting into a detailed examination of how operations and the feeling of space are affected over the life of the healthcare facility.
Following is an excerpt from a PowerPoint presentation on costs:
REMEMBER!
- Design costs = 0, 1 units
- Capital cost = 1 unit
- Maintenance costs (first 25 y) = 100 units
- Running costs (first 25 y) = 400 units”
The flip side of the debate, given by Sameer Mehta, Director Projects in Hosmac India Pvt. Ltd., a leading Healthcare Facility Design and Management Firm in Mumbai India:
The argument is presented well. How does one put a value to efficiency?
But the moot point is, a small reduction in grid does result in a not- so-insignificant saving….aside of saving on ground coverage, a constraint we often are forced to contend with. See the table below. Take a floor plate of 30,000 sq ft. If we reduce the grid matrix from 8 m to 7.2 m, one saves nearly 6,000 sq ft. Take four floors, and one is looking at a saving of 24,000 sq ft!
| Particulars | L | B | Area |
| Area in sq ft | 200 | 150 | 30,000 |
| Area in sq m | 61 | 46 | 2,789 |
| Particulars | L | B | Area |
| @ grid of 8 m | 7.6 | 5.7 | 44 |
| Reduced area on conversion of grid to 7.2 m | 54.9 | 41.2 | 2,259 |
| Area reduced by (in sq m) | 530 | ||
| Area reduced by (in %) | 19% |
Aside of the civil costs, it also translated into reduced HVAC and electrical loads, not to speak of reduced maintenance costs. Not too sure what the PPT extract implies. If only one were able to put a value to the efficiency compromised by doing so, one might have made a valiant attempt. Sorry for being a spoilsport in the case for a larger grid….just had to present the other side.
Not at all, Sameer. We value your thoughts on the matter.
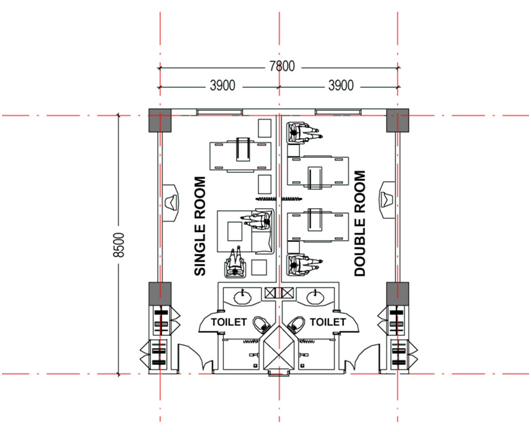
Please note Sameer’s figures are based on a reduction from 8.00 M to 7.20 M, which is somewhat more than the reduction of grid as a statement about the niche market that the hospital wants to address.. Note also that he has shrunk the grid in both directions, while we can shrink only in one. It is never possible to shrink on the other side if we are going with the concept of flexi-single-twin-share and 6-bed wards on the same grid. Please see the part plan below. But of course this holds good only for the inpatient ward footprint. Grids outside this footprint can be shrunk. Still, it presents another point of view. The argument may not be totally one-sided.
Sameer too admits that it is difficult to put a value to the loss in hospital operations efficiency with a smaller grid. We also cannot quantify the loss in “feeling of space”, smaller lobbies and less waiting area. But if we cannot quantify it, it does not mean it does not exist. We have to use our imagination to the best extent possible.
Sameer asks about the relevance of the PowerPoint extract. I think we should ask ourselves that after a hospital has been operating for 25 years how many CEO’s have wished that the promoters had spent 1.25 units on the initial cost. (or, closer to home, 0.125 units on design!)
However, a good point he makes is the reduction in HVAC load and electrical load that would occur with the shrinking of the grid. Energy saving will bring down that 400 units after 25 years. We have to strike a balance between these various design factors that are pulling us in opposite directions.
I have a suggestion. Let us reduce the grid from 7.50 M to 7.20 M and then value engineer the project, maybe with the help of a professional consultant in the field(Remember: 0.125 units on design!) But who will pay for this little relevant piece of research?
In conclusion, an excerpt from an article on flexibility in healthcare facility design:
If we considered the ultimate in flexibility to be “disposable” buildings and, during planning, assumed a
15-year facility life span (as we might for equipment or hardware), then we could avoid writing this
article. Instead, we assume a building has a 50-year life span and take the attitude that buildings are
too costly to tear down. Should the driving motivation be the cost to operate the services rather than
the cost of the building?
I leave you thinking about that one.
Bibliography:
Concepts in Flexibility in Healthcare Facility Planning, Design and Construction
Tannis Chefurka and Faith Nesdoly, Partners, RPG-Resource Planning Group Inc. and John Christie,
Director, Parkin Architects
157 thoughts on “Grid-Shrinking as a means of Cutting Costs in Healthcare Facility Design:A Conversation”