Flexible Design Principles in Healthcare Facility Planning
vis-a-vis
Adaptive Alternative Usage
• Healthcare facilities as designed and built in India today would be resistant to change of use
• However, “flexibility” as a design objective in contemporary healthcare facility design worldwide is of paramount importance
• This flexibility refers only to flexibility of change of alternative diagnostic, therapeutic and interventional medical procedures
• Inpatient accommodation still remains relatively inflexible even today
• Flexibility in terms of planned adaptive alternative usage would be a different concept altogether
• This concept is not even addressed in current architectural debate or writing, it is a non-issue
• What could be a possible planned alternative usage for a typical 250-bed multi-specialty hospital?
• To answer this question, it is necessary to understand the four broad constituent parts of such a hospital
o Inpatient accommodation
o Diagnostic/Therapeutic/Interventional medical areas
o Public and Support areas
o Building Services and Staff areas
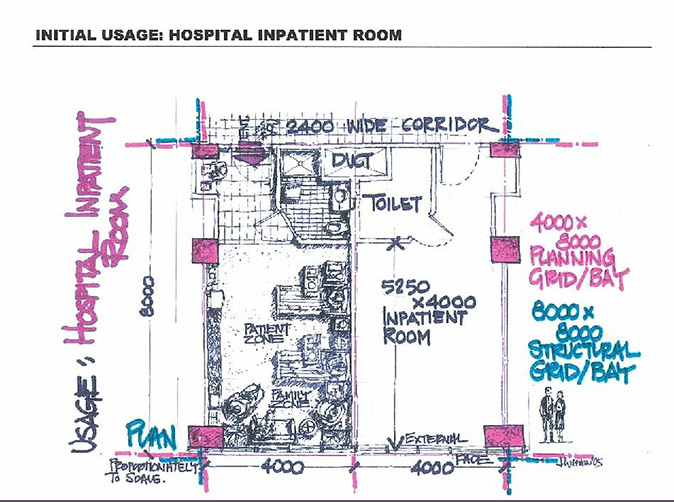
• Inpatient Accommodation: It’s purpose and characteristics
o Houses inpatients before and after medical procedures typically in single, twin-share or 4 to 6 bed wards
o Major architectural characteristics are the need for an external wall window for view and natural light and the need for attached toilets (in today’s healthcare market)
o Accessed through a minimum 8′-0″ wide corridor necessary for stretcher movement
o Typically occupies the uppermost floors of the hospital
• Diagnostic/Therapeutic/Interventional Medical Facilities: Their purpose and characteristics
o To perform medical procedures and investigations, for consultation and therapy
o Major architectural characteristics are rooms custom-designed for hi-tech equipment, complex space planning needs resulting in atypical layouts, only large open areas being waiting areas, if at all
o Typically occupy the Ground to Second or Third Floor of the hospital
• Public and Support areas: Their purpose and characteristics
o Public areas such as the Main Entrance Lobby, Cafeteria and Auditorium
o Support areas such as Main Kitchen, Laundry and Central Sterilization
o Major architectural characteristics are easily understood for Public areas, Support areas are largely mechanized
o Support areas such as Administration offices, IT and Communication hubs
o Typically scattered throughout the above-mentioned lower floors, some areas may be in the basement
• Building Services and Staff areas: Their purpose and characteristics
o Building Services such as HVAC Plant room, Electrical room etc.
o Major architectural characteristics are that they are typically over -sized as air-conditioning and electrical loads are higher than other common building types
o Typically housed in the basement or in a separate service building, site permitting
•Planned Alternative Usages possible:
o Hotel
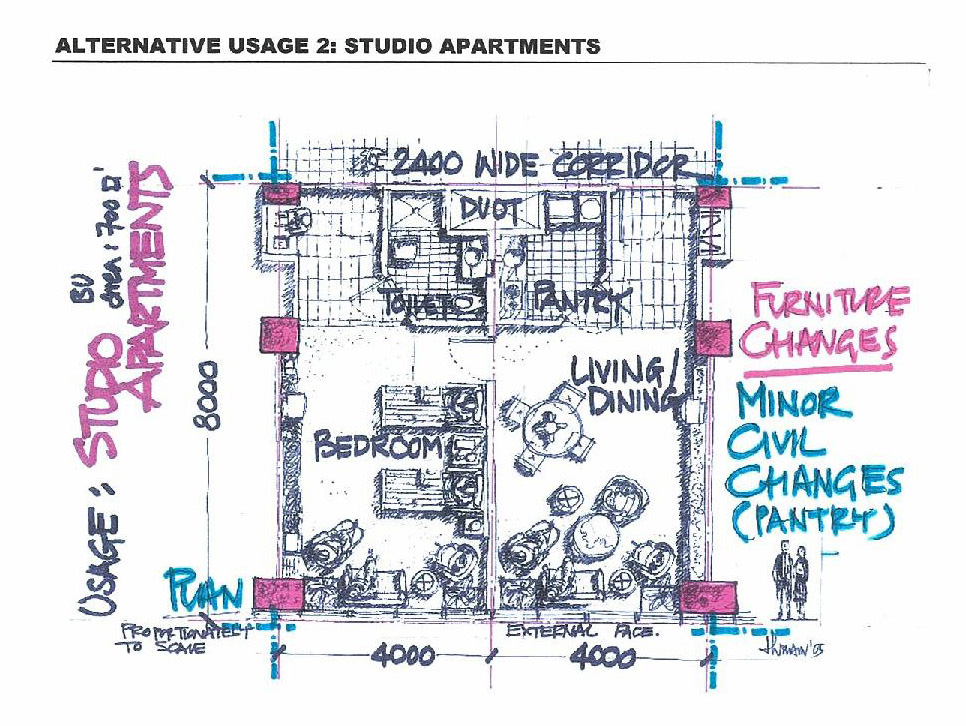
o Combination of Service Apartments (upper floors) and Hypermarket (lower floors)
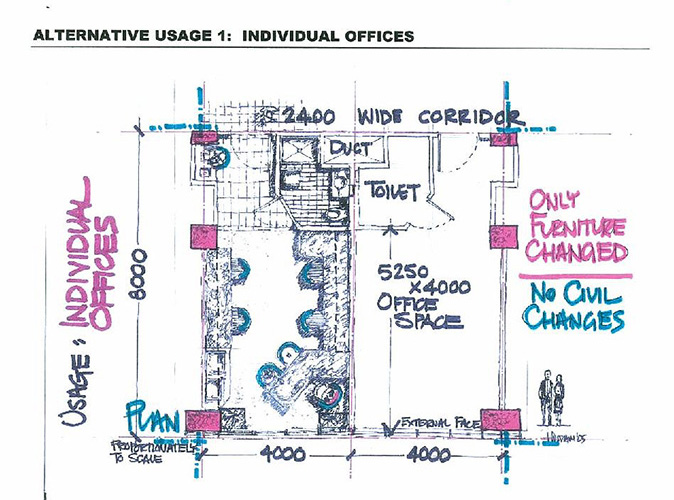
o Self-contained offices (upper floors) of up to 350 square feet BUA including attached toilet and Software Park (lower floors)
o Work ability of alternative usage will be a location specific choice
• What would be the impact on initial planning of the hospital for such planned adaptive reuse?
o The upper floors, i.e. the inpatient accommodation, could be planned to be adaptively reused
with little to no planning impact on the hospital inpatient rooms initially provided, for the above -mentioned new facilities.
o The lower floors would need major planning constraints imposed on the initial
hospital design to work for the adaptive reuse mentioned above
o Building services should present no hindrance to this planned reuse as they
would be over -designed for any possible reuse
o Provision for parking would need to be considered for the alternative use planned from the onset
• Typical Planning grid for hospitals in India – approx. 4.0 M x 8.0 M (i.e. 13′-0″ x 26′-0″)
o One planning grid would contain one inpatient room + attached toilet
o Two planning grids together would form the structural grid i.e. 8.0 M x 8.0 M
o This planning grid is derived from the configuration of the inpatient floors
• The area requirement for the total hospital (BUA for 250 -bed multi -specialty) will be
1000 to 1200 square feet / inpatient bed (depending on market positioning and pricing). This area would be all inclusive, except for covered parking.
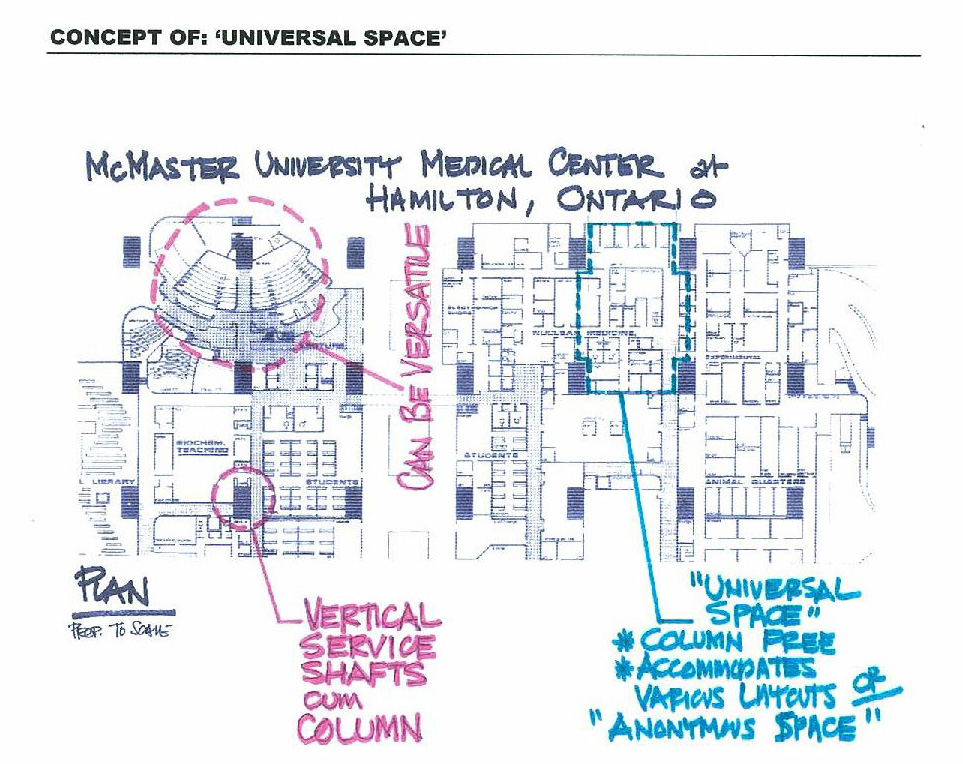
• How then would we plan the lower floors to make this adaptive reuse possible?
o A possible solution could be systematized infrastructure and building structures (e.g., those used at McMaster University Medical Center in Hamilton, Ontario)
o The concept is one of “universal space”. This consists of large, modular blocks of space with integrated structure/ service shafts at regular intervals and a system of building services layout that would incorporate “reserved rights -of way” for all building services so that they could be
delivered to any point in the building.
o Slabs would be designed to support walls at all points, as is standard practice in hospital design anyway.
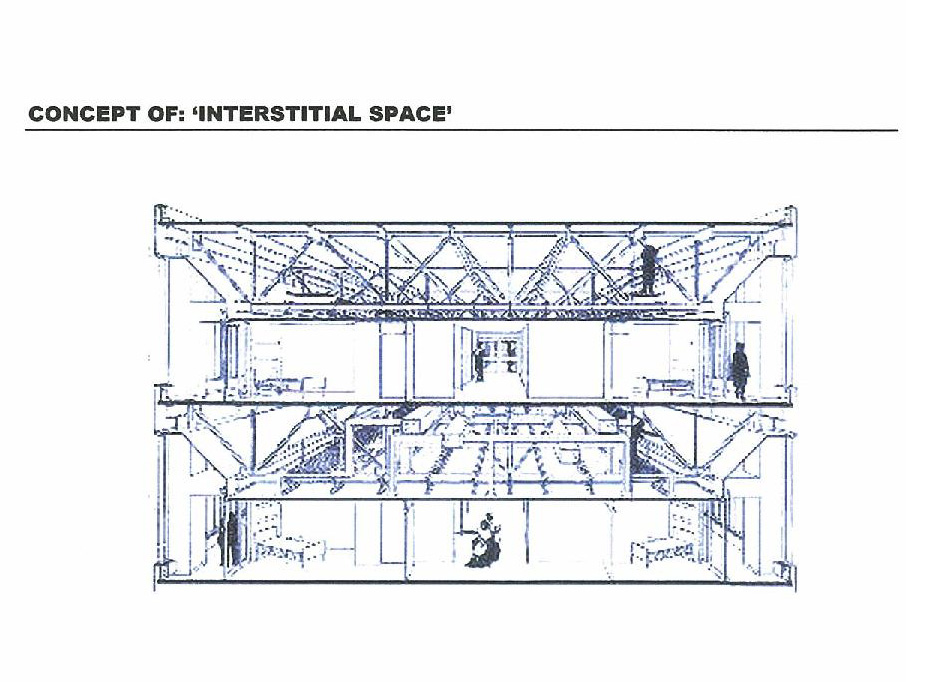
• What would be the cost implications of this built-in flexibility for adaptive reuse?
o In the Indian context, it could be high.
o It involves the concept of interstitial space to accommodate a super -grid or large, column -free space with limited structural constraints on the planning and changes to the floor plates
o The increased capital cost must seem justified to provide the organization with this type of flexibility
• How else could we find solutions to this problem?
o If we could decide on the type of adaptive reuse that is desired, both “before” and “after” designs could be prepared prior to construction and the cost implications could be
quantified for feedback into the design process until a satisfactory design/initial cost for the desired flexibility is achieved
o If the site permits, selective demolition combined with new construction could be an answer, but this approach would be site specific, could not be a generalized solution
• In conclusion…
o Remember, in the long run, operating costs will quickly far exceed capital costs. Flexibility provided for adaptive reuse works as flexibility for a successfully running
hospital as well, which needs it just as much, if not more.
o In the ideal world, the perfect balance can be found between functionality of the space and the generic parameters that afford its flexibility. Construction rupees can be optimized. In the real world, this point of balance may seem elusive, but teamwork, attention to detail, and open communications throughout the planning and design process will help us close in on our target. Our multi -disciplinary
planning and design team possesses the knowledge and skills necessary to create the dynamic and long-term solution that is desired.
Appendix
• Typical Building Services Requirements for a 250 -bed Multi -Specialty Hospital
o Water Tank capacity = 800 to 1000 liters //) (-9 / ))/)”,
o 2000 to 3000 KVA of power plus/minus 100% D.G. Set back-up
o HVAC = thumb rule calculation 1 TR / 200 square feet BUA. HVAC requirements
will be more complex in terms of 100% fresh air requirements, HEPA (High Energy Particulate Arrestors) filters for maintenance of sterile conditions in the OT Suite, Laboratories, Intensive Care Units and Central Sterilization. Installed HVAC capacity will be in excess for alternative usages.
o Typically, hospitals do not require Hi -Speed Broadband connectivity that would be required for alternative usages like Software Parks or Office space.
Pingback: Google